Table of Contents
Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised
Clinical Opiate Withdrawal Scale
Service End, Discharge and Discharge Follow-up
Detoxification Assessment
GENERAL Tab
The user gathers information about why the client is presenting for services and documents that information in the General section. The data fields and questions under the General tab are the same for all clients receiving all service types and of any age.
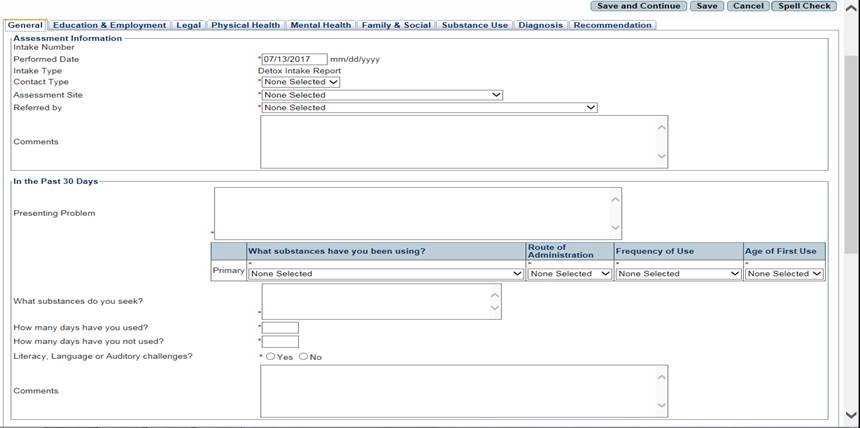
ASSESSMENT INFORMATION
Assessment Number (Generated by the CMBHS System)
Each assessment completed for a client and documented in CMBHS has a unique assessment number generated by the system. It is view only and cannot be changed by the User.
Assessment Date
- The user records the date that the client was assessed. The system will default to the current day’s date.
- If the assessment occurred on some other date before the current date, the user can change this field to the correct date. A future date cannot be entered.
- If the assessment interview occurred on more than one day, enter the first date that the assessment interview began.
- The system requires a full date using either of the following two formats: mmddyyyy or mm/dd/yyyy. When you enter the date using the mmddyyyy format (eight numbers with no slashes), the system automatically reformats and displays the date as mm/dd/yyyy.
- CLICK IN the text box and TYPE IN the information.
Assessment Type
The system will auto-fill according to the Assessment Type (Initial, Update, Service End or Discharge) that you chose from the dropdown list. This is a view-only field and cannot be changed by users.
Contact Type
The user documents the contact type that best describes how the Assessment interview was conducted with the client. CLICK ON one of the options available:
· Face to Face
· Telehealth
· Telephone
Assessment Site
The user documents the setting where the Assessment interview took place with the client. Information may have been obtained from the client or collaterals in several settings. Answer this question indicating where the majority of the contact with the client occurred.
· Select the assessment setting that best describes where the interview(s) took place.
· CLICK ON one of the items in the dropdown box:
|
Ambulance, Land |
Boarding Home |
|
Community IMD |
Community setting (Community Mental Health Center) |
|
Correctional Facility |
Custodial Care Facility |
|
Emergency Room |
General medical hospital |
|
Group Home |
Home |
|
Hospice |
Hospital |
|
Independent Laboratory |
Inpatient Hospital |
|
Inpatient Psychiatric Facility |
Jail |
|
Mobile |
Mobile/Extended/Outreach |
|
Not Applicable |
Nursing facility |
|
Office/Clinic |
Other |
|
Outpatient Hospital |
Psychiatric Facility Partial Hospitalization |
|
Psychiatric Residential Treatment Center |
Residential Substance Abuse Treatment Facility |
|
School |
Service facility |
|
State Mental Health Facility |
State Mental Retardation Facility |
|
State funded community hospital |
State or Local Public Health Clinic |
Referral Source. This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. The user documents who referred the client to the provider for services.
CLICK ON one of the referral source options:
|
Community Health Service |
Community Mental Health Services |
|
Court Services/DWI/DUI |
Department of Family Protective Services (Adult or Child Protective Services) |
|
Drug Court |
Family/Friend |
|
Hospital (Community) |
Hospital (State) |
|
Insurance/Employee Assistance Program |
Outreach, Screening, Assessment, and Referral (OSAR) |
|
Peer Support/Recovery Support |
Probation/Parole |
|
School |
Self (Client) |
|
Substance Use Disorder Prevention/Intervention/ Treatment |
Work/Employer |
|
Community Service Provider (local, state, federal ) |
|
Comments
The user may enter comments in this box that relate to the Assessment Information fields. Only include information that relates to these fields.
· Comments will be entered into the client’s health record and will be seen by those that have the authority to view this part of the record. Under some circumstances, this may include the client. Always consider the consequences of entering sensitive information such as HIV status.
· This comments text box is optional.
· CLICK IN the text box and TYPE IN the information.
In the past 30 days
Presenting Problem
Document reason the client presented for services clearly and concisely in the client’s own words.
Substance Table
Primary, Secondary and Tertiary
This field contains a required element from the Treatment Episodes Data Set Minimum Data Set.
· If the client uses one drug, select answers in the row labeled Primary. If the client does not use one drug select None and the remainder of the items will not be required fields.
· If the client uses two drugs, fill in the fields on the Primary and Secondary rows.
· If the client uses three drugs, fill in the fields on the Primary, Secondary and Tertiary rows.
· If the client uses four or more drugs, fill in the fields on the Primary, Secondary and Tertiary rows and put information about the other drugs used by the client in the Comment text box.
Primary
What substances have you been using? - Answer the following question about the primary drug that the client uses in the first cell of the table.
· Select the Primary Substance Used by the client from the dropdowndropdown list.
· You may select a specific drug or a group of drugs, based on how much information is available and whichever best describes the drug the client uses.
· For substance abuse services, the client must have a “primary” drug used documented.
Route of Administration. This field contains a required element from the Treatment Episodes Data Set Minimum Data Set.
· Select the answer choice that represents how the client gets the substance into his/her body.
· The answer choices are:
§ Oral
§ Inhalation
§ Injection
§ Smoking
§ Other
· CLICK ON the blue arrow to the right of the dropdown box and CLICK ON your answer and move to the next cell.
· If the client uses more than one route of administration, select the usual route of admission.
· If you select Other, document the Other route of administration used by the client in the comments text box.
Frequency of Use. This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. Document how frequently the client uses this drug by selecting one of the answer choices from the dropdown list.
· CLICK ON the blue arrow to display the answer choices. The answer choices for this question are:
§ No use in past month
§ 1-3 times in the past month
§ 1-2 times in the past week
§ 3-6 times in the last week
§ Daily
Age at First Use
What was the client’s age when they first used this drug? CLICK ON one of the options available:
Select from the following choices:
§ <8
§ 8
§ 9
§ 10
§ 11
§ 12
§ 13
§ 14
§ 15
§ 16
§ 17
§ 18
§ 19+
For drugs other than alcohol, these fields contain the age at which the client first used the respective substance. For alcohol, these fields record the age of first intoxication.
Secondary
· If the client uses a secondary substance, select the Secondary Substance used by the client from the dropdown list. If you select a substance on the row in the table labeled Secondary, then all the fields in that row will be required fields. See the above instructions for Route of Administration, Frequency of Use, and Age at First Use.
· If the client does not use a secondary substance, you may leave all the fields blank.
Tertiary
· If the client uses a third substance, select the Tertiary substance used by the client from the dropdown list. If you select a substance on the row in the table labeled Tertiary, then all the fields in that row will be required fields. See the above instructions for Route of Administration, Frequency of Use, and Age at First Use.
· If the client does not use a third substance, you may leave all the fields blank.
What substances do you seek? This field displays only if
there are drugs listed in the table. It is a mandatory field. Use this text
field to document the drugs the client seeks whether it is one of the drugs
listed or another drug. The user documents substances that the client sought if
the preferred substance(s) was not available or accessible to the client. CLICK
IN the text box and TYPE IN the information.
How many days have you used? How many days have you not used? Answer both items. The sum of the answers cannot exceed 30. This text field denotes the days of use within the past 30 days of any non-prescribed or non-misused prescription substance. CLICK IN the text box and TYPE IN the information.
Comments Add additional information about the client’s substance use in the available text box. This comments text box is optional. CLICK IN the text box and TYPE IN the information.
Literacy, language or auditory barriers? Document language, literacy, or auditory barriers and issues that the client may have. CLICK IN the Yes or No radio button to answer.
Comments Add additional information about the client’s need for accommodation in the treatment setting in the available text box. This comments text box is optional.
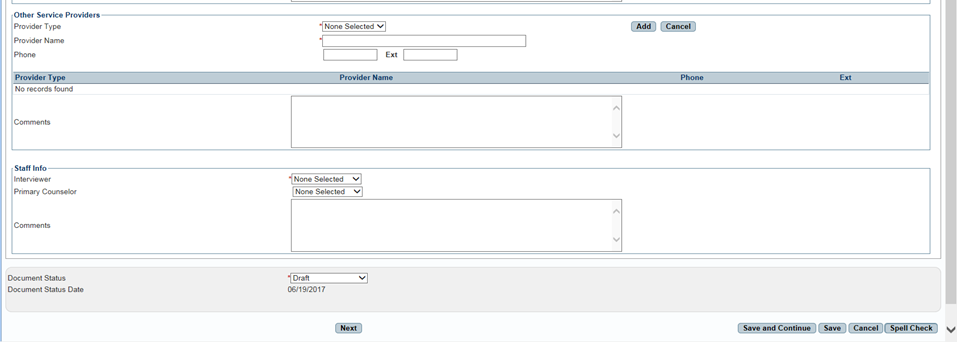
OTHER CURRENT SERVICE PROVIDERS The interviewer identifies who provides the client with recovery support, community services, treatment or guidance for their physical, mental, emotional, or spiritual health. The user documents information from the client, and collateral sources as appropriate, to document other service providers. Adding Other Service Providers is not required. However, if you click on the New Service Provider button, the fields in the detail screen will display required fields.
To enter Other Service Providers CLICK ON the New Service Provider button to access the detail screen. CLICK ON the arrow to the right of the Provider Type box this field defaults to “None Selected”. CLICK ON the provider type that best describes the provider’s services. Click IN the Provider Name field and type the name. Click IN the Phone field and type the phone number. CLICK ON the add button to add the information. The user may add as many service as needed.
|
CAUTION: |
|
Provider Type
The answer choices for this question are:
|
Provider Type |
Provider Type Description |
|
MH |
A traditional provider of Mental Health Services to include a Psychologist, Social Worker, or Marriage & Family Therapist. May be a publicly or privately employed individual or group practice. |
|
SA |
Traditional provider of Substance Abuse Services. May be a publicly or privately employed individual or group practice. |
|
Medical |
A traditional Medical practitioner to include a physician or nurse, or home health agency. May be a publicly or privately employed individual or group practice. |
|
Dental |
A dentist, orthodontist, or dental surgeon. May be a publicly or privately employed individual or group practice. |
|
Alternative |
A “non-traditional” service provider that may not be part of the mainstream culture but may represent the beliefs of an ethnic or cultural minority or sub-group. |
|
Spiritual |
Qualified representative, clergy or lay, who spiritually supports, counsels and guides the client. Includes but is not limited to priests, rabbis, ministers, and imams. |
|
Psychiatry |
A medical doctor practicing as a psychiatrist. |
|
Legal |
An attorney or other person licensed to provide legal services. |
|
Other |
Person providing services to the client that does not fit into any of these categories. |
· If you select Other as an answer, document what type of service is provided in the Comments text box below the table.
· CLICK IN the text box and TYPE IN the information.
Provider Name Document the Provider’s credentials if available. This text field is optional. CLICK IN the text box and TYPE IN the information.
Comments Add comments about the client’s support system in the available text field. This comments text box is optional.
STAFF INFO (Information)
Interviewer
The name of the user who first created and started documenting the Assessment will display in this field as the default.
· If the name that displays is not that of the person who actually interviewed the client, the name must be changed.
· CLICK ON the dropdown menu to search for the name of the person who interviewed the client.
· Select the name by highlighting it and CLICK ON the name.
Primary Counselor
The system will the display the name of the assigned primary counselor. If the client has not been assigned a primary counselor, no name will display.
Comments Add comments in the available text box related to staff information. This comments text box is optional.
EDUCATION & EMPLOYMENT Tab
Users document information about the client’s education and employment in this section.
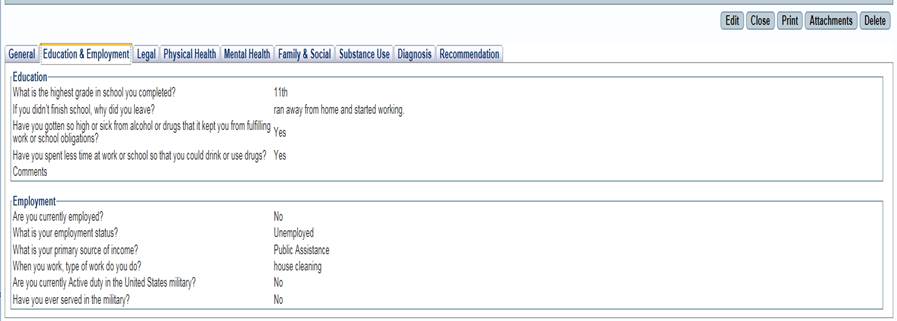
EDUCATION Section
What is the highest grade in school you completed? This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. This question is Life History Screening question. Answers to the life history screening questions result in the display of options for modifications to treatment on the Recommendation Tab. See the full description of modification to treatment on the Recommendation tab. CLICK ON one of the options available that best represents the client’s answer.
· <6
· 6
· 7
· 8
· 9
· 10
· 11
· 12
· Bachelor
· Master
· Certification
· Other
If you didn’t finish school, why did you leave? This question is a Life History Screening question and displays for adult clients only. Answers to life history screening questions result in the display of options for modification to treatment on the Recommendation tab. See the full description of modification to treatment on the Recommendation tab. CLICK IN the text box and TYPE IN the information. Type In the available text box a summary of the client’s response
Have you gotten so high or sick from alcohol or drugs that it kept you from fulfilling work or school obligations? The answer is used in the Severity Score calculation. Please see full description of the severity score calculation in the Diagnosis tab section. The answer is used in the Dimension Calculator for the ASAM Recommended Course of Treatment. Please see full description of the Dimension calculation in the Recommendation tab section. CLICK IN the Yes or No radio button.
Have you spent less time at work or school so that you could drink or use drugs? The answer is used in the Severity Score calculation. Please see full description of the severity score calculation in the Diagnosis tab section. The answer is used in the Dimension Calculator for the ASAM Recommended Course of Treatment. Please see full description of the Dimension calculation in the Recommendation tab section. CLICK IN the Yes or No radio button.
EMPLOYMENT Section (Education & Employment tab)
Are you currently employed? CLICK IN the Yes, No, or N/A radio button.
What is your employment status? This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. The user documents the client’s employment status at the time of admission. CLICK ON one of the items in the dropdown list. The options in the dropdown list are:
|
Full time |
36-40 hours per week including active duty members of the uniformed services |
|
Part time |
1-35 hours a week |
|
Unemployed |
0 hours a week; Looking for work during the past 30 days or on layoff from employment |
|
Not in Labor Force |
Not looking for work during the past 30 days or a student, homemaker, disabled, retired or an inmate of an institution. |
|
Unknown |
Client doesn’t know how to answer this item |
Reason for Not In Labor Force? This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. This item displays if the answer is “Not in the Labor Force” to the question “What is your employment status?” CLICK ON one of the items in the dropdown list. The options in the dropdown list are:
|
Disabled |
Client has a formal status as “Disabled” established by declarations from doctors and documented as such with Social Security or the Office Veteran Affairs. |
|
Homemaker |
Client is the primary person taking care of the dwelling and the occupants of the dwelling. |
|
Inmate |
Client was in a legally secured facility that keeps a person, otherwise able, from entering the labor force. |
|
Retired |
Client worked and formally retired from the labor force. |
|
Student |
Client attends school in any form. |
|
Seasonal Worker |
Client only works during specific times of the year. |
|
Other |
The client’s reason for not being in the labor force does not meet any of the criteria described in the list. |
|
Not Applicable |
|
What is your primary source of income? This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. The user documents the client’s principal source of financial support. CLICK ON one of the items in the dropdown list. The options in the dropdown list are:
· Disability
· Public Assistance
· Retirement/pension
· Wages/Salary
· Other
· None
When you work, what type of work do you do? This question is optional. CLICK IN the text box and TYPE IN the information.
Are you currently active duty in the United States military? This question displays for adults only. CLICK IN the Yes or No radio button.
Have you ever served in the military? This question displays for adults only. This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. CLICK IN the Yes, No, N/A radio button.
LEGAL Tab
The user documents the client’s current legal status.
Current Information
What is your current legal status? CLICK ON one of the items in the dropdown list. This question is optional. The options in the dropdown list are:
· Jail or Prison
· Probation
· Parole
· Diversion Program
· Awaiting Trial
· Awaiting Sentencing
· NA
In the past 30 days, how many times have you been arrested? This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. This question is a Life History Screening question. Answers to life history screening questions result in the display of options for modification to treatment on the Recommendation tab. See the full description of modification to treatment on the Recommendation tab. TYPE a number in the available text box. Maximum characters are two. If the client had more than 96 arrests in the last 30 days, TYPE 96 in the text box and provide additional information in the Comments text box.
Would you like assistance with your legal status? CLICK IN the Yes or No radio button.
Comments Enter any additional information about the client’s legal issues that are relevant to requested services. This comments text box is optional. CLICK IN the text box and TYPE IN the information.
PHYSICAL HEALTH Tab
The user documents answers to medical questions specifically related to Substance Use Disorder symptoms and potential co-occurring medical conditions that may increase the severity of the consequences of substance use. The Clinical Opiate Withdrawal Scale (COWS) and Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-AR) display when the client is receiving services in a Detoxification setting. The COWS will display only for clients with Opioid withdrawal diagnoses. The CIWA-AR will display only for clients with Alcohol Withdrawal diagnoses. The COWS and CIWA are available in the blank forms independent of the Detoxification Assessment for use by contractors during detoxification services.
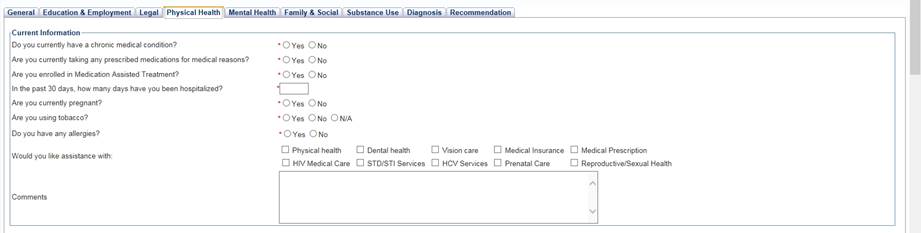
CURRENT Health
Do you currently have a chronic medical condition? CLICK IN the Yes or No radio button.
If yes, explain. The system displays this question when the answer is yes to “Do you currently have a chronic medical condition? Type in the available text box clear and concise information about the client’s chronic health issues that impact the client’s services.
Are you currently taking any prescribed medications for medical reasons? CLICK IN the Yes or No radio button.
If yes, what are they? The system displays this question when the answer is yes to “Are you currently taking any prescribed medications for medical reasons?” TYPE IN the available text box clear and concise information about the client’s medications.
Are you enrolled in Medication Assisted Treatment? This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. The answer “yes” to this item will result in this field displaying on the client’s treatment or service plan. CLICK IN the Yes or No radio button.
Are you prescribed any of the following? This field will only display if the answer to “Are you enrolled in Medication Assisted Treatment?” is yes. CLICK ON one of the items in the dropdown list. The options in the dropdown list are:
· Naloxone
· Suboxone
· Methadone
· Subutex
· Buprenorphine
· Vivitrol
Have you recently stopped prescription use of Vivitrol (naltrexone), methadone, or buprenorphine (Suboxone, Subutex)? Yes or No. CLICK IN in the Yes or No radio button. The answer to this item is used in the Priority Population calculation.
Have you experienced a non-fatal overdose? Yes or No. CLICK IN the Yes or No radio button. The answer to this item is used in the Priority Population calculation.
If “yes” then, have you ever been administered naloxone or Narcan? This question displays when the answer is yes to “have you experienced a non-fatal overdose?” CLICK IN in the Yes or No radio button. The answer to this item is used in the Priority Population calculation.
In the past 30 days, how many days have you been hospitalized? Type a number in the available text box. Maximum characters are two. If the client had more than 96 hospitalizations in the last 30 days, Type 96 in the text box and provide additional information in the Comments text box.
Have you given birth in the past 18 months? CLICK IN Yes or No. Click in the Yes or No radio button. And the next question displays only when the client profile choices are “Female”.
If “yes” then, have used opioids in the past 3 years? This question displays when the answer is yes to “Have you given birth in the past 18 months?” CLICK IN in the Yes or No radio button. The answer to this item is used in the Priority Population calculation.
Are you currently pregnant? This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. This field specifies whether the client was pregnant at the time of admission. This question and the next question display only when the client profile choices are “Female”. CLICK IN the Yes or No radio button.
Do you think you could be pregnant? This item only displays if the answer is no to “Are you currently pregnant?” CLICK IN the Yes, No, or Unknown radio button.
Are you using tobacco? CLICK IN the Yes or No radio button.
Would you like assistance to cut back or quit? This question is only displayed, and is required, if you answered YES to “Are you using tobacco?” This field generates a tobacco cessation referral. CLICK IN the Yes or No radio button.
Do you have any allergies? CLICK IN the Yes or No radio button.
If yes, what are they? This question is only displayed, and is required, if you answered YES to “Do you have any allergies?” CLICK IN the text box and TYPE IN the information. TYPE IN the available text box clear and concise information about the client’s allergies that impact the client’s services.
Would you like assistance with: CLICK IN the box next to each item a service for which the the client would like to receive assistance. These are referrals that can be entered into the Referral screens to assist the client’s course of treatment or discharge support.
· Physical health
· Dental health
· Vision care
· Medical Insurance
· Medical Prescription
· HIV Medical Care
· STD/STI Services
· HCV Services
· Prenatal Care
· Reproductive/Sexual Health
Comments TYPE IN the available text box any additional information obtained during the interview with the client that relates to physical health issues relevant to the delivery of services.
The following two assessment scales will only display in the Detoxification Assessments.
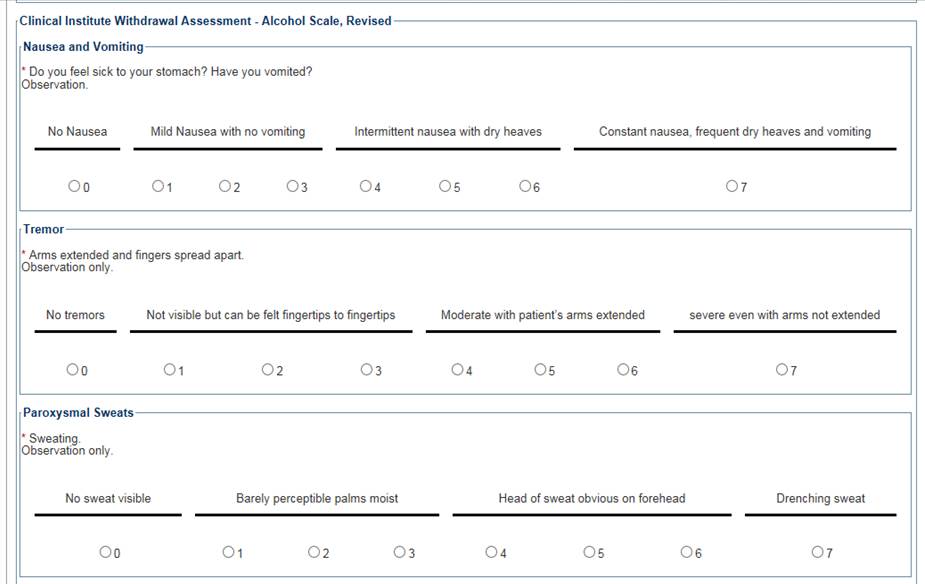
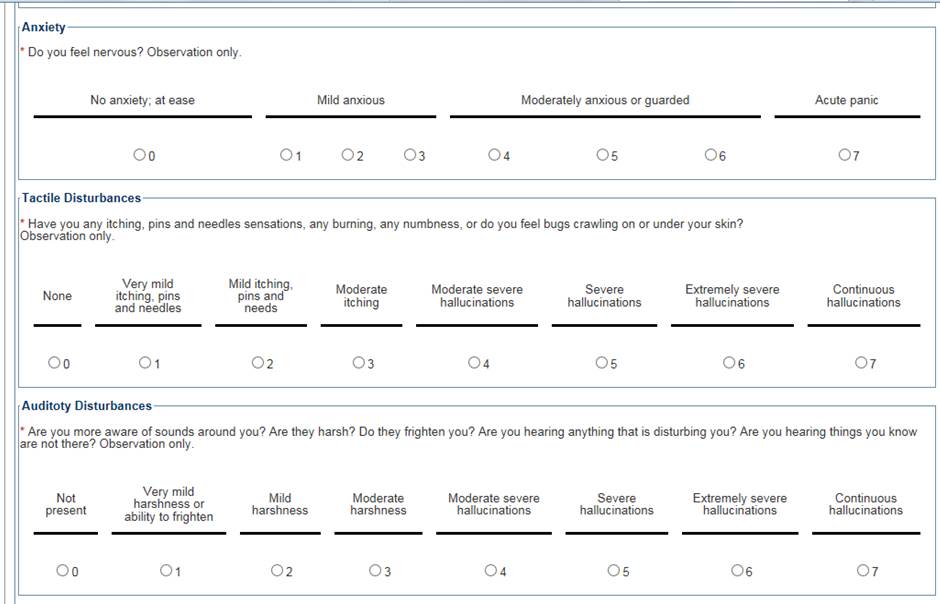
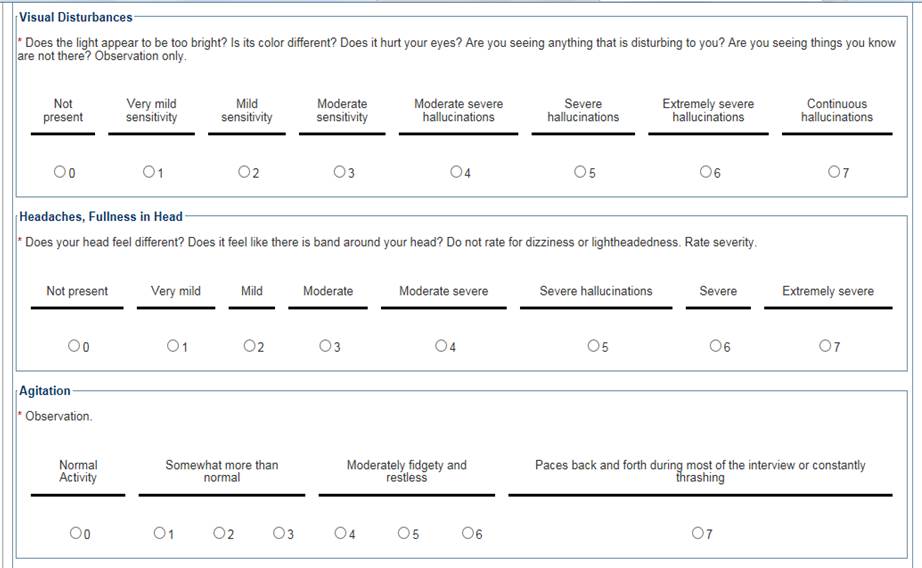
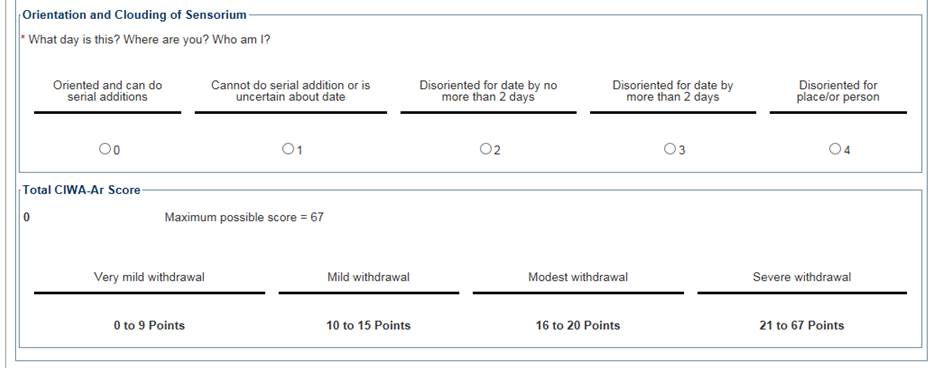
Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised
CLICK ON the radio button that best describes the client’s symptoms. The system will calculate the score.
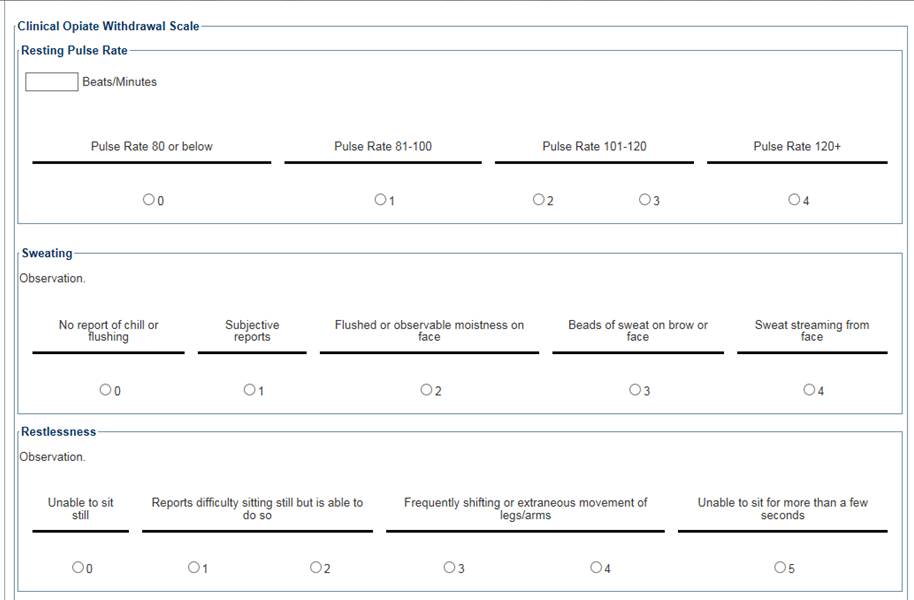
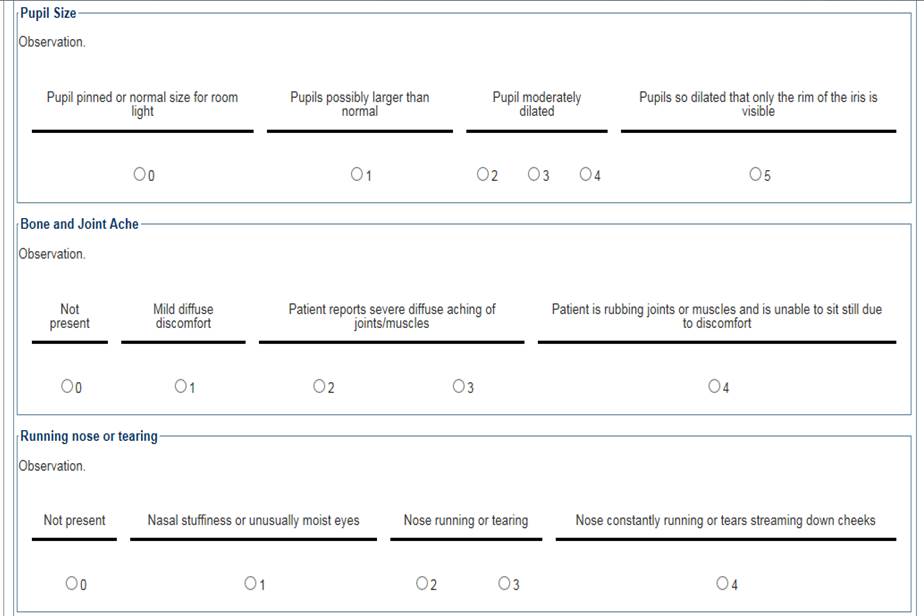
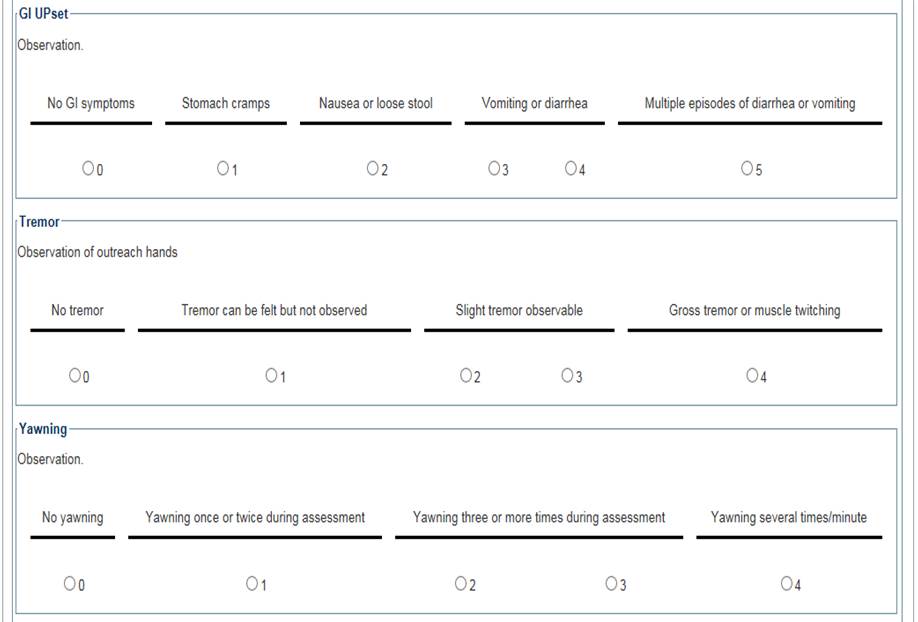
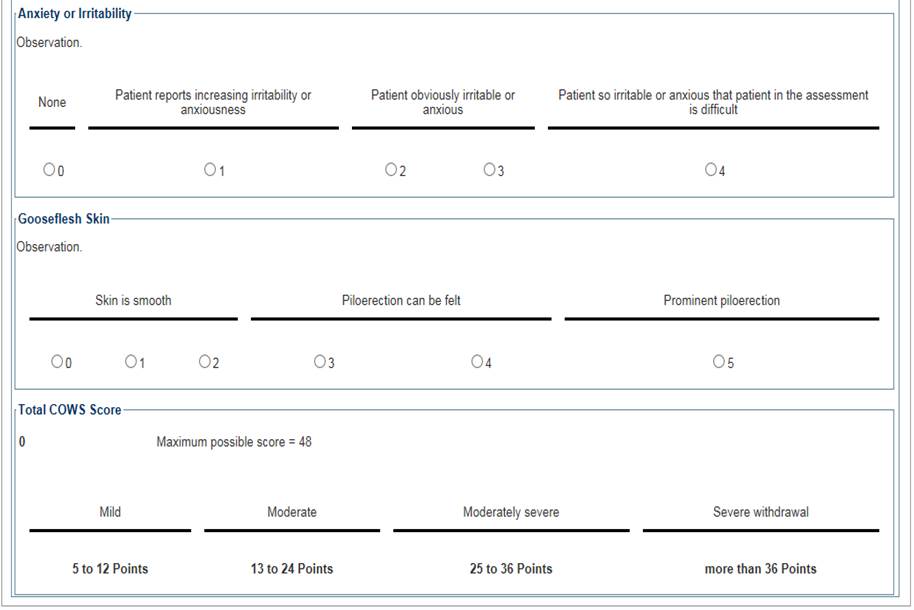
Clinical Opiate Withdrawal Scale
CLICK IN the box and type the number that that best describes the client’s heart beats per minute. Then CLICK ON the radio button that represents the range.
For all other items, CLICK ON the radio button that best describes the client’s symptoms. The system will calculate the score.
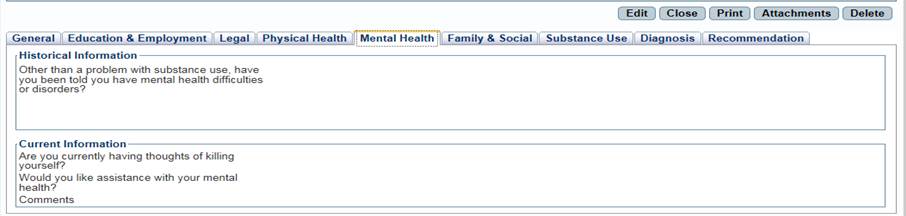
MENTAL HEALTH Tab
Clinicians document information about the client’s mental health when the client is not under the influence of mind-altering substances in this section. During the interview, Clinicians need to ensure the client understands that the symptoms describe on this tab represent things that happen when the client is not under the influence of mind altering substances. The information gathered is historical and current information.
Historical Information
Other than a problem with substance use, have you been told you have mental health difficulties or disorders? This question is a Life History Screening question. Answers to life history screening questions result in options for modification to treatment on the Recommendation tab. See the full description of modification to treatment on the Recommendation tab. CLICK IN the Yes or No radio button.
If yes, what were you told: This field displays when the answer is yes to “Other than a problem with substance use, have you been told you have mental health difficulties or disorders? “CLICK IN the text box and TYPE IN the information. (text box 250 characters)
Are you currently having thoughts of killing yourself? This question screens for suicide risk factors. This question is optional. CLICK IN the Yes or No radio button
Would you like assistance with your mental health? This question is optional. CLICK IN the Yes or No radio button
Comments. This text field is for additional mental health comments. This comments text box is optional. CLICK IN the text box and TYPE IN the information.
FAMILY & SOCIAL Tab
Users document information about the client’s family, social and living environment in this section.
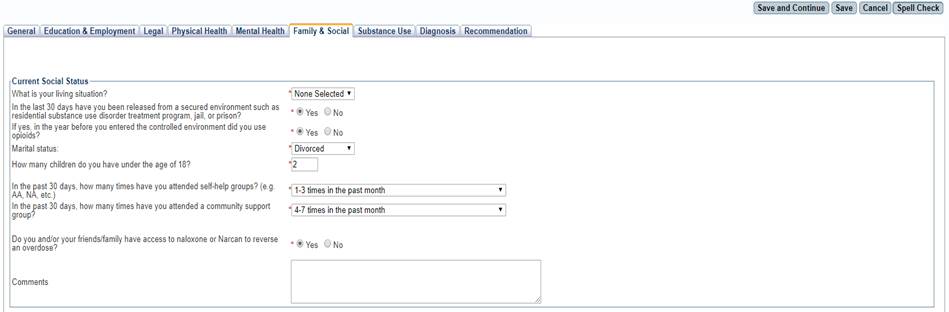
Current Social Status
What is your living situation? This field contains a required element from the Treatment Episodes Data Set Minimum Data Set. This field contains the client’s living status including homeless, living with parents, in a supervised setting or living on his or her own. This question is a Life History Screening question. Answers to life history screening questions result in the display of options for modification to treatment on the Recommendation tab. See the full description of modification to treatment on the Recommendation tab.
CLICK ON one of the options available:
|
Term |
Treatment Episodes Data Set Minimum Data Set definition |
|
Dependent |
Clients living in a supervised setting such as a residential institution, halfway house, or group home, and children under the age of 18 living with parents, relatives, or guardians or in foster care |
|
Independent |
Clients living alone or with others without supervision |
|
Homeless |
Clients with no fixed address; includes shelters |
In the last 30 days have you been released from a secured environment such as residential substance use disorder treatment program, jail, or prison? CLICK ON in the Yes or No radio button.
If yes, in the year before you entered the controlled environment did you use opioids? This question displays when the answer is anything other than yes to the question “In the last 30 days have you been released from a secured environment such as residential substance use disorder treatment program, jail, or prison?” CLICK IN in the Yes or No radio button. The answer to this item is used in the Priority Population calculation.
Marital status:
This field contains a required element from the Treatment Episodes Data Set Minimum DataSet.
This field contains client’s marital status.
|
Divorced |
|
|
Never Married |
Includes clients whose only marriage was annulled |
|
Now Married |
Includes those living together as married |
|
Separated |
Includes those separated legally or otherwise absent from spouse because of marital discord |
|
Widowed |
|
How many children do you have under the age of 18? CLICK IN the text box and TYPE IN the information.
In the past 30 days, how many times have you attended self-help groups? (e.g. AA, NA, etc.)
This field contains a required element from the Treatment Episodes Data Set Minimum Set.
This field contains the number of times the client has attended a self-help group in the past 30 days preceding the date of admission to detoxification services. CLICK ON one of the options available:
· No attendance in the past month
· 1-3 times in the past month
· 4-7 times in the past month
· 8-15 times in the past month
· 16-30 times in the past month
· Some attendance in the past month, but frequency unknown
In the past 30 days, how many times have you attended a community support group? This field contains the number of times the client has attended a community support group in the past 30 days non-affiliated with substance use services. CLICK ON one of the options available:
· No attendance in the past month
· 1-3 times in the past month
· 4-7 times in the past month
· 8-15 times in the past month
· 16-30 times in the past month
· Some attendance in the past month, but frequency unknown
Do you and/or your friends/family have access to naloxone or Narcan to reverse an overdose?
CLICK IN in the Yes or No radio button.
Comments. This text field is for additional living situation and family dynamic comments. This comments text box is optional. CLICK IN the text box and TYPE IN the information.
SUBSTANCE USE Tab
Users document information about the client’s substance use in this section.
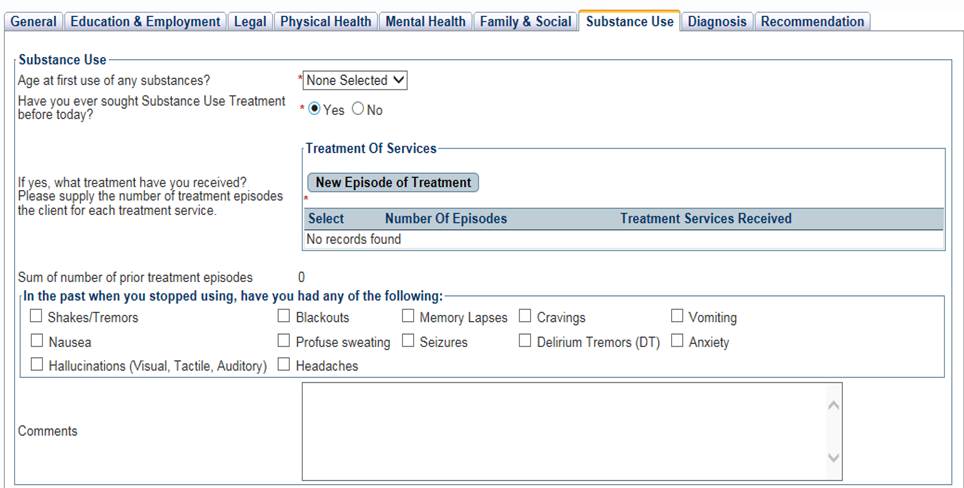 Substance Use
Substance Use
Age at first use of any substances? CLICK ON one of the options available:
· <6
· 6
· 7
· 8
· 9
· 10
· 11
· 12
· 13
· 14
· 15
· 16
· 17
· 18
· 18+
Have you ever sought Substance Use Treatment before today? CLICK IN the Yes or No radio button
The table is conditional and only displays if the answer is yes to “Have you ever sought Substance Use Treatment before today?”
Number of Episodes
Treatment Services Received. CLICK ON to select client Treatment Received
· Residential Detoxification Services (ASAM Level 3.7 Withdrawal Management)
· Ambulatory Detoxification Services (ASAM Level 2 Withdrawal Management)
· Intensive Residential Services (ASAM Level 3.5 Clinically Managed - Intensity Residential Services)
· Supportive Residential Services (ASAM Level 3.1 Clinically Managed – Low Intensity Residential Services)
· Outpatient Services (ASAM Level 1 Outpatient Services)
· Outpatient Services (ASAM Level 2.1 Intensive Outpatient Services)
· Medically Assisted Treatment for substance use
Sum of number of prior treatment episodes. This field contains a required element from the Treatment Episodes Data Set Minimum Data Set.
Comments This text field is for additional historical detoxification comments. This comments text box is optional. CLICK IN the text box and TYPE IN the information.
DIAGNOSIS Tab
Strengths and Limitations
TAC 25 Part 1 Chapter 448 Subchapter H Rule 448.803 Assessment requires for a description of client’s strengths and weaknesses as well as a comprehensive list of client’s problems, needs and strengths for each assessment.
Client's Strengths CLICK IN the text box and TYPE IN the information.
Client's Limitations CLICK IN the text box and TYPE IN the information.
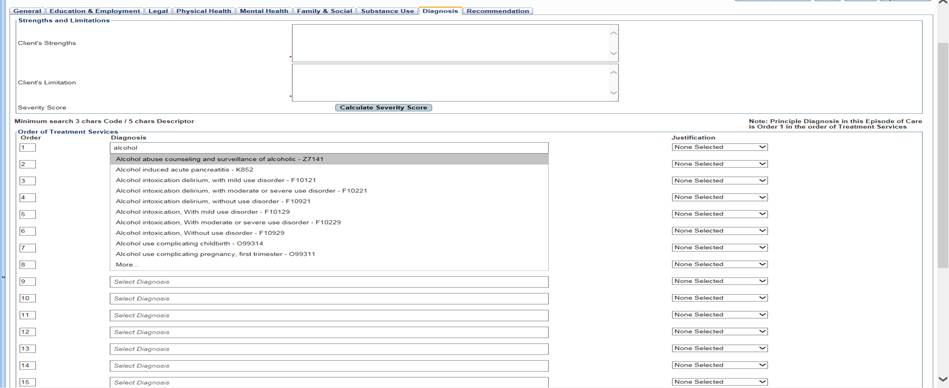
The selection of diagnoses is done in the rows displayed. The clinician may enter up to 18 diagnoses. The clinician needs to ensure the diagnosis associated with the number one (1) is the diagnosis being treated. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM), the diagnosis being treated is referred to as the Principal Diagnosis. The clinician may arrange the numbers next to each line in the order of treatment services. The calculated severity will be display only based on the diagnostic-related questions throughout the assessment. The diagnostic-related questions can be found on the physical health, mental health, family and social, and substance use tabs. The system will rearrange the diagnosis so they are displayed in the order the clinician selected when the clinician adds the diagnoses. To add the diagnosis or diagnoses, the clinician needs to CLICK ON the Add button.
Order of Treatment Services table
The search method allows the clinician to type in three characters associated with the code or five characters associated with the diagnosis description. The system will display all the codes related to the information typed in the row. The clinician needs to CLICK ON the code the represents the diagnosis supported by the symptoms discovered during the assessment which match the criteria in the DSM.
Justification CLICK ON the option that describes the reason the diagnosis code was selected.
· By client report
· By clinician observation
· By collateral report
· By history
· By impression
· By physician report
Comments This text field is for additional diagnostic comments. This comments text box is optional. CLICK IN the text box and TYPE IN the information.
RECOMMENDATIONS Tab
![]()
Priority Population Status
View Only (Explain calculation and show formula with questions associated)
· Pregnant Injecting Drug User
· Pregnant Substance User
· Injecting Drug User
· High Risk for Overdose
· Referred by DFPS
· Priority Population Designation Not Met
The table below shows the items used to calculate the status of Priority Population
|
|
Priority Population Label and Items in the SU Initial Assessment |
Scores used in the Calculator |
|
|
Pregnant and Injecting |
|
|
Tab |
Questions |
Answers |
|
General tab |
Route of administration? The answer to this item is used in the Priority Population calculation. |
Answer: Injection =1 |
|
General/Historical Health: |
Are you currently pregnant? The answer to this item is used in the Priority Population calculation. |
Answer: Yes = 1; No = 0 |
|
|
Do you think you could be pregnant? The answer to this item is used in the Priority Population calculation. |
Answer: Yes = 1; No = 0 |
|
|
Pregnant |
Answer: Yes = 1; No = 0 |
|
Tab |
Question |
Answers |
|
General/Historical Health |
Are you currently pregnant? The answer to this item is used in the Priority Population calculation. |
Answer: Yes = 1; No = 0 |
|
|
Injecting |
|
|
Tab |
Question |
Answers |
|
General tab |
Route of administration? The answer to this item is used in the Priority Population calculation. |
Answer: Injection =1 |
|
|
High Risk for Overdose |
Answer: Yes = 1; No = 0 |
|
Tab |
Questions |
Answers |
|
Current Health |
Have you recently stopped prescription use of Vivitrol (naltrexone), methadone, or buprenorphine (Suboxone, Subutex)? |
Answer: Yes = 1; No = 0 |
|
|
Have you experience a non-fatal overdose? |
Answer: Yes = 1; No = 0 |
|
|
If “yes” then, have you ever been administered naloxone or Narcan? This question displays when the answer is yes to “Have you experienced a non-fatal overdose?” |
Answer: Yes=1 ; No = 0 |
|
|
Have you given birth in the past 18 months? |
Answer: Yes=1; No=0 |
|
|
If “yes” then, have you used opioids in the past 3 years? This question displays when the answer is yes to “Have you given birth in the past 18 months?” |
Answer: Yes = 1; No = 0 |
|
|
DFPS |
|
|
Tab |
Question |
Answers |
|
General tab |
Referral Source |
Answer: DFPS =1 |
Client Support Needs

The items on display are all the items listed on all the tabs. The interviewer or clinician needs to check the boxes associated with every item for which the client requested assistance. The clinician may edit any item on the original tab. Questions that resulted in a checked box will remain the same.
|
Tab |
Support Need |
|
General |
Language or Auditory |
|
Education & Employment |
Education, GED, Employment, Veterans Affairs |
|
Legal |
Legal |
|
Physical Health |
Tobacco, Physical Health, Dental Health, Vision Care, Medical Insurance, Medical Prescription, HIV Medical Care, STD/STI Services, HCV Services, Prenatal Care, Reproductive/Sexual Health |
|
Mental Health |
Mental Health |
|
Family Social |
Reunification Services, Living Situation, Family Support, Housing Environment, Paying for Housing, Community Support, Financial Assistance Programs, Child Welfare System, Social Welfare Programs, Sober Living Environment, Recovery Coach, Support Group, Food Assistance, Transportation Assistance, Children’s Services and Needs |
Comments This text field is for additional client support needs comments. This comments text box is optional. CLICK IN the text box and TYPE IN the information.
Service End, Discharge and Discharge Follow-up
The Service End and Discharge Detoxification assessments have the same items displayed as the Detoxification Intake. There are many answers carried forward for the user. These items can be edited if the client’s information changes. There are other items that must be answered with new information from the client. The required items are displayed with the red asterisk *. The Discharge Follow-up Detoxification assessment has fewer items from the initial assessment than the other assessments. Some items have language that is a little bit different. The required items will be displayed with the red asterisk *.